Basic HTML Version




37
Blunt injury thoracic aorta & endovascular treatment,
Idla et al.
www.angiologia.pl
(debranching) was performed as follows: crossover from
the right aCC (common carotid artery) to the left aCC
with a supported ePTFE 8 mm graft (IMPRA, Carboflo,
C. R. Bard, Inc). Also, transposition of the proximal
part of the left aCC to the left subclavian artery was
performed. As a second step, a new endoprosthesis,
a Zenith TX2 (Z-Trak-Plus), 32 × 200 mm (Cook, Inc.,
Bloomington, IN), was inserted via the right common
femoral artery following the same endovascular princi-
ples as described above. Angiography was performed
via right brachial artery with a diagnostic pigtail catheter.
After the implantation of the Zenith TX2 endograft
(covering left aCC), a type I endoleak was still noted,
and balloon-dilatation of the proximal part of the endo-
graft with CODA balloon (Cook, Inc., Bloomington, IN)
was performed. After the dilatation no endoleak was
detected (Figure 5).
The patient’s recovery was uneventful and he was
discharged on the 15th postoperative day.
One year later a planned follow-up control CT-an-
giography showed patent crossover PTFE vascular graft.
There were no endoleaks of the endograft (Figure 6).
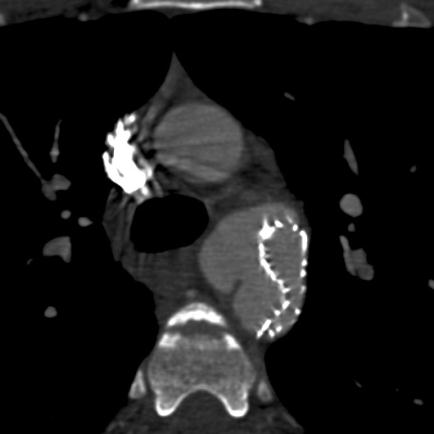
Figure 3A, B.
Type I endoleak was described by CT-angiography; the pseudoaneurysm was filled with the contrast medium; the
length of lip of the endograft was measured as 15 mm
A
B
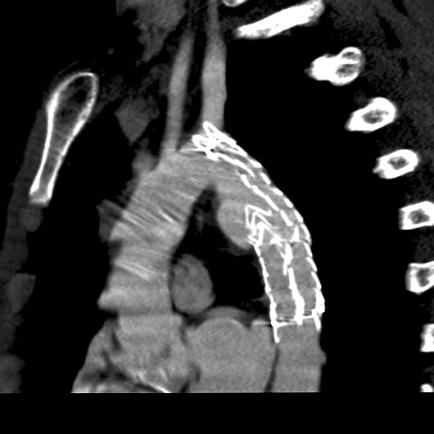
Figure 4A, B.
Collapse of the endograft (Gore TAG 26 x 100 mm) was observed by CT-angiography
A
B