Basic HTML Version




36
Acta Angiol, 2012, Vol. 18, No. 1
www.angiologia.pl
North Estonia Medical Centre. After the first emergency
operation (splenectomy and sutures of the liver) and
stabilisation of the patient, CT-angiography revealed
multifractures of the facial bones, contusion of the lungs,
and blunt traumatic injury of the descending thoracic
aorta (according to the classification by Schumacher
— please see Figure 1 legend) [5] (Figure 1).
Description of TEVAR
(thoracic endovascular aortic repair)
The right common femoral artery was exposed
surgically. A standard angiographic pigtail catheter
was inserted through a percutaneous puncture (5Fr)
into the contralateral common femoral artery to per-
mit angiographic control throughout the procedure.
A 260-cm, 0.035-inch Terumo guidewire (Terumo
Medical Corporation, Tokyo, Japan) was placed, un-
der fluoroscopic control, into the ascending aorta
through a sheath in the common femoral artery, and
a 5F measuring pigtail catheter was advanced into the
ascending aorta over the Terumo guide. This pigtail
catheter was used to exchange the Terumo guide
wire for a 0.035-inch-diameter Lunderquist (Cook,
Inc., Bloomington, Ind) to guide the passage of the
20F sheath facilitated by the application of a small
amount of mineral oil. Gore TAG (W.L. Gore and As-
sociates, flagstaff AZ) 26 × 100 mm endograft (second
generation) deployment was performed under flu-
oroscopic control; the orifice of the subclavian artery
was covered. A control angiography was performed,
and no obvious endoleaks were detected. Finally,
the introducer was removed from the groin, and the
arteriotomy was sutured (Figure 2).
A type I endoleak was noted on the CT-angiogra-
phy 36 hours later (Figure 3). The balloon-dilatation of
the proximal part of endograft was performed via the
left common femoral artery with a Tri-Lobe balloon
(W.L. Gore and Associates, Flagstaff AZ). A minor
endoleak (I type) in region of the inner curve of the
aortic arch was still detected. Subsequently, a conse-
rvative treatment strategy was chosen, and the patient
recovered under anti-hypertensive and antibacterial
treatment. The patient was discharged on the 24th
postoperative day.
Repeated endografting of the aortic arch
Due to a moderate chest pain the patient was ad-
mitted to our hospital three weeks later. New CT-
-angiography showed the collapse of the GORE-TAG
endograft (but no occlusion of the thoracic aorta) (Figure 4).
As a first step, supra-aortic branch revascularisation
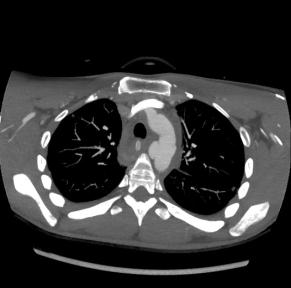
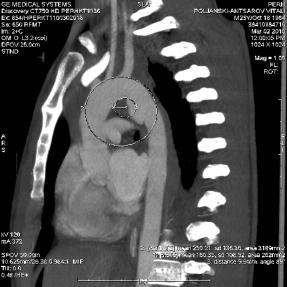
Figure 1A, B, C.
CT-angiography showed the traumatic dissection in the region of the aortic isthmus. IIC class according to
Schumacher
is characterized as traumatic dissection, no complete aortic laceration with active haemorrhage, the pseudoaneurysm
is developing. Radius of inner curve of the aortic arch is 3.4 cm; the diameter of the aorta is 20 mm
A
B
C
Figure 2.
Aortography immediately after employment of the
Gore TAG (26 × 100 mm)