IMAGE IN CARDIOVASCULAR MEDICINE
Cardiology Journal
2024, Vol. 31, No. 6, 931–932
DOI: 10.5603/cj.99859
Copyright © 2024 Via Medica
ISSN 1897–5593
eISSN 1898–018X
A rare presentation of disseminated micronodular melanoma masquerading as an infiltrative cardiomyopathy
Mariana Martinho1* João Mirinha Luz1*Bárbara Ferreira1Inês Cruz1Oliveira Baltazar1Diogo Santos Cunha1Filipe Nogueira2Patrícia Lima3Ana Catarina Gomes1Hélder Pereira14
João Mirinha Luz1*Bárbara Ferreira1Inês Cruz1Oliveira Baltazar1Diogo Santos Cunha1Filipe Nogueira2Patrícia Lima3Ana Catarina Gomes1Hélder Pereira14 1Cardiology Department, Hospital Garcia de Orta, Almada, Portugal
2Pathologic Anatomy Department, Hospital Garcia de Orta, Almada, Portugal
3Oncology Department, Hospital Garcia de Orta, Almada, Portugal
4Centro Cardiovascular da Universidade de Lisboa, Centro Academico Medico de Lisboa, Universidade de Lisboa, Lisboa, Portugal
Address for correspondence: Mariana Martinho, Cardiology Department, Hospital Garcia de Orta, Avenida Torrado da Silva, 2805–267 Almada, Portugal, tel: +351 913024081, e-mail: mariana.martinho6@gmail.com
*Both authors contributed equally to the paper
Received: 19.03.2024 Accepted: 18.10.2024
This article is available in open access under Creative Common Attribution-Non-Commercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) license, allowing to download articles and share them with others as long as they credit the authors and the publisher, but without permission to change them in any way or use them commercially.
Keywords: melanoma, micronodular infiltration, heart failure, infiltrative cardiomyopathy, imaging
A 62-year-old woman presented a one-month history of right heart failure symptoms, without fever, or respiratory or consumptive symptoms. Blood tests revealed low high-sensitivity troponin T of 63 ng/dL and N-terminal pro-brain natriuretic peptide of 7806 pg/mL. A chest X-ray with an increased cardiothoracic ratio and bilateral parenchymal miliary opacities was followed by a transthoracic echocardiogram, revealing marked biventricular and interatrial septum hypertrophy, severe pericardial effusion (maximum 20 mm in diastole) with signs of pre-tamponade, such as swinging heart, 21% mitral E wave respiratory variation, and impaired diastolic filling of the right atrium (Suppl. Video 1). Thoracic computed tomography (CT) confirmed countless lung micronodules, mediastinum-hilar lymphadenopathy, and polyserositis, suspicious of tuberculosis. Pericardiocentesis led to clinical improvement, and etiological tests were inconclusive (adenosine deaminase value in pericardial fluid was 3.0 U/L, reference < 40 U/L, with negative C-reactive protein for tuberculosis). Positron emission CT showed multisystemic hypermetabolic foci and cardiac magnetic resonance-confirmed tumoral infiltration and intracavitary thrombi, managed with anticoagulation (Fig. 1). Ultrasound-guided biopsy of an axillary node identified melanoma metastasis. The patient died 22 days after admission.
Approximately 50% of melanomas spread to the heart and pericardium, but ante-mortem diagnosis is rare due to its silent nature. Multisystemic and cardiac dissemination typically show a macronodular “solid pattern”, leading to obstructive symptoms or embolization. The initial presentation as an infiltrative cardiomyopathy due to micronodular infiltration is rare and has never been described. This case demonstrates the value of multimodality cardiac imaging and a multidisciplinary approach to allow for timely diagnosis and therapy.
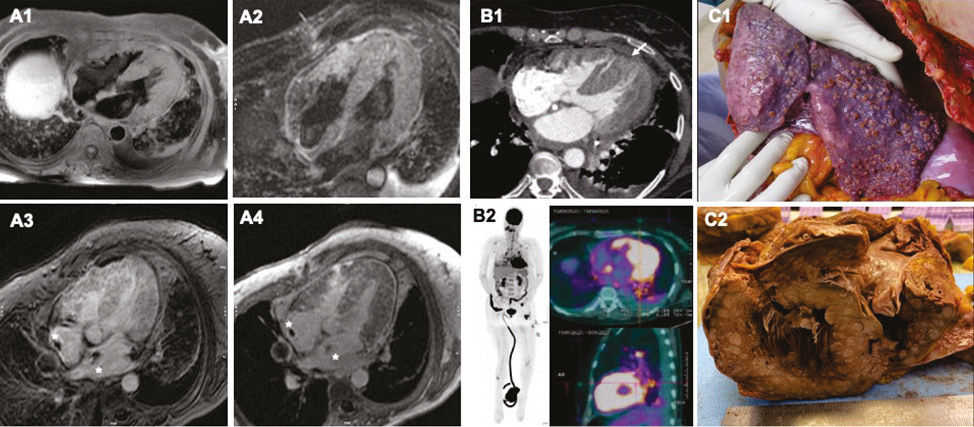
Figure 1. Panel A depicts cardiac magnetic resonance imaging, with markedly hypertrophied ventricles, and a heterogenous mass in the right ventricle free-wall and intracavitary thrombi (white asterisks). There is signal hyperintensity in T1-weighted sequences (double IR FSE with fat saturation in panel A1) and hyperintensity in T2-wighted sequences (triple IR FSE, panel A2). Moreover, there is heterogenous uptake in early and late gadolinium enhancement studies (panel A3 and A3, respectively). Panel B1 depicts the chest computed tomography (CT) with marked biventricular hypertrophy and interatrial septum thickening (white arrow and asterisk, respectively), with myocardial heterogenous appearance. Panel B2 shows multiple hypermetabolic foci in the maximum intensity projection (MIP) image in 18F-FDG positron emission tomography (PET), along with myocardial hypermetabolism in the PET/CT fusion images. Panel C refers to the macroscopic autopsy findings, where multiple dispersed sub-centimetric nodular lesions are seen in the left lung (panel B1) and in a cross-section of the cardiac ventricles (panel B2), revealing extensive infiltration of the myocardium, papillary muscles, and pericardial adipose tissue
Conflicts of interest: None declared.
Funding: None declared.
Supplementary material: Video 1. Parasternal long-axis view of transthoracic echocardiogram. Marked hypertrophy of the left ventricle (LV) walls, with isoechoic and granular-appearing myocardium. There is normal segmental contractility, LV function, and left valves morphology and function. Significant circumferential pericardial effusion, characterized by clear fluid appearance, along with apparent mild systolic and end-diastolic collapse of the RV free wall.


