Interventional cardiology
IMAGE IN CARDIOVASCULAR MEDICINE
Cardiology Journal
2024, Vol. 31, No. 1, 179–180
DOI: 10.5603/cj.97144
Copyright © 2024 Via Medica
ISSN 1897–5593
eISSN 1898–018X
Veno-arterial extracorporeal membrane oxygenation circuit as second vascular access for transcatheter aortic valve replacement
Raphaël Giraud123 Benjamin Assouline123Nils Perrin4Karim Bendjelid123Stéphane Noble24
Benjamin Assouline123Nils Perrin4Karim Bendjelid123Stéphane Noble24 1Intensive Care Unit, Geneva University Hospitals, Geneva, Switzerland
2Faculty of Medicine, University of Geneva, Switzerland
3Geneva Hemodynamic Research Group, Geneva, Switzerland
4Department of Internal Medicine, Division of Cardiology, Geneva University Hospitals, Geneva, Switzerland
Address for correspondence: Raphaël Giraud, MD, PhD, Intensive Care Unit, Geneva University Hospitals, Rue Gabrielle Perret-Gentil 4, CH-1211 Geneva, Switzerland, tel: +41 79 553 21 96, fax: +41 22 382 74 70, e-mail: Raphael.Giraud@hcuge.ch
Received: 30.08.2023 Accepted: 19.01.2024
This article is available in open access under Creative Common Attribution-Non-Commercial-No Derivatives 4.0 International (CC BY-NC-ND 4.0) license, allowing to download articles and share them with others as long as they credit the authors and the publisher, but without permission to change them in any way or use them commercially.
A 65-year-old man, known for stage-IV chronic obstructive pulmonary disease and high gradient severe aortic stenosis presented with respiratory failure secondary to heart failure. Echocardiography showed a reduced left ventricular ejection fraction (25%) and a mean gradient at 23 mmHg. The patient developed multiple organ failure with acute renal failure, hepatic cytolysis and pulmonary edema requiring intubation.
A computed tomography scan showed an aortic root compatible with transcatheter aortic valve replacement (TAVR) (calcium score: 6161 HU) (Fig. 1A, C). The vascular access assessment showed significant stenosis of the right iliac artery and both subclavian arteries. It was decided to urgently perform transfemoral TAVR under veno-arterial-extracorporeal membrane oxygenation (ECMO) considering the patient’s hemodynamic and respiratory instability.
Both femoral arteries were punctured under echo-guidance. Balloon dilation of the right iliac artery stenosis was performed before the 14F-eSheath insertion (Fig. 1D–G). The 15F-arterial ECMO cannula was inserted through the left femoral artery.
The second vascular access required during TAVR procedure (i.e.; for aortic root angiogram) was performed through the ECMO circuit tubing at the segment of the reinjection cannula using the Seldinger technique to insert a 6F-sheath (Fig. 1B). No bleeding was observed around the sheath.
After the Sapien-3 implantation, the ECMO circuit was briefly clamped and the portion of the ECMO cannula with the 6F-sheath was cut (Fig. 1B). Finally, the ECMO circuit was reconnected and unclamped.
The puncture of the ECMO circuit tubing at the segment of the reinjection cannula to obtain an arterial vascular access is feasible and safe.
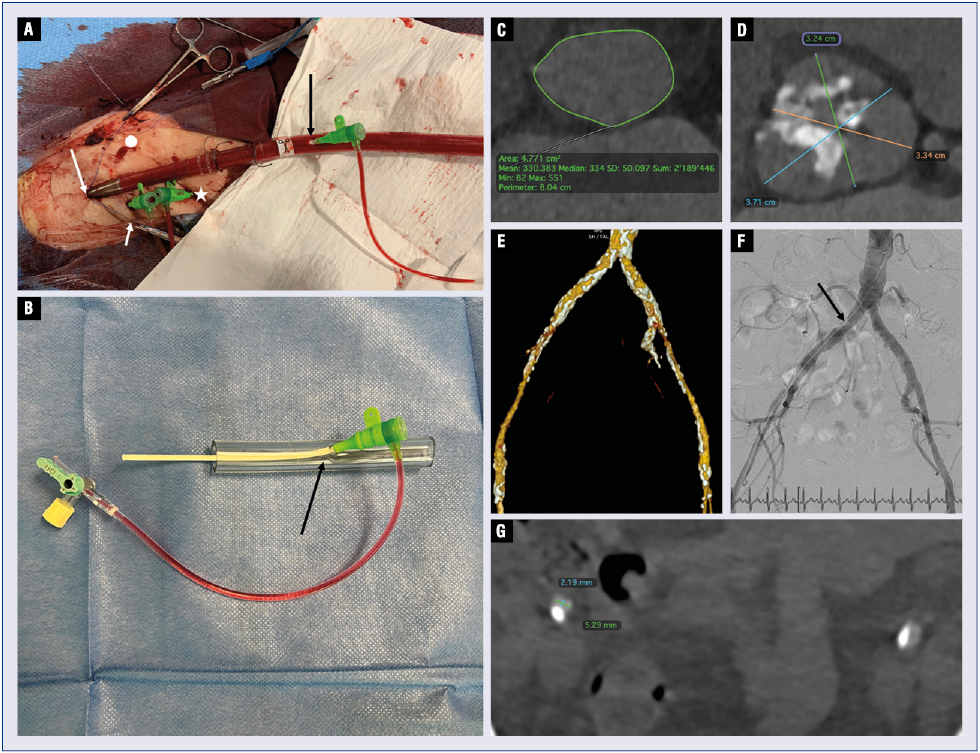
Figure 1. A. A 6F Terumo femoral introducer sheath (black arrow) was introduced in the circuit proximal to the connection to the arterial canula using a regular 18 G Seldinger Angiokard needle and a regular 0.35 wire. 6F-sheath inserted in the femoral vein (short white arrow). Reperfusion canula of the extracorporeal membrane oxygenation (ECMO) circuit inserted in the superficial femoral artery (white asterisk). 15F-ECMO reinjection canula access pre-closed using two ProStyle (white dot); B. Portion of the ECMO circuit with the 6F-sheath cut from the ECMO circuit (black arrow); C. Annulus sizing using the OsiriX software; D. Sinus of Valsalva measurements using the OsiriX software (green: left-, yellow: right- and blue: non-coronary cusps); E. Computed tomography scan three-dimensional reconstruction of the aorto-ilio-femoral vascular bed showing extensive calcification (white plaques); F. Aorto-ilio-femoral aortography showing severe calcified stenosis of the right common iliac artery; G. Measurement of the right common iliac artery.


